Dr S K Gupta,MD,Consultant Physician Hospital, New Delhi
Scenario of G B Syndrome outbreak Now in India
- As of January 29, 2025, Maharashtra has reported a total of 127 suspected cases of Guillain-Barré Syndrome (GBS), with two suspected fatalities.
- Among these, 72 cases have been confirmed.
- The affected regions include Pune Municipal Corporation (23 cases), newly added villages in the PMC area (73), Pimpri Chinchwad Municipal Corporation (13), Pune Rural (9), and other districts (9). Currently, ~20 patients are on ventilator support.
- In addition, Kolkata has reported two GBS-related deaths.
Health authorities are on site to investigate the situation
- Authorities investigating ◆contaminated water being a suspected source.
- Samples of stool and blood of those infected are being tested at the NIV Pune lab, but yet to get any definite leads on the cause behind the spread.
What has been Found
- Campylobacter jejunum bacteria was found in 4 stool samples that were collected from 21 GBS patients in Pune.
- Norovirus was found in some cases who had diarrhea
{ However according to the medical literature norovirus doesn’t lead to GBS}
- Water samples from different parts of the city have been sent for chemical and biological analysis to the Public Health Laboratory.
Mechanism of GBS:
- GBS occurs when antimicrobial antibodies, created to fight bacterial or viral infections like Campylobacter jejuni or respiratory infections, cross-react with the myelin sheath protein of peripheral nerves.
Symptoms
- Flaccid weakness predominates in most patients with Guillain-Barré syndrome; it is always more prominent than sensory abnormalities and may be most prominent proximally.
- Relatively symmetric weakness with paresthesias usually begins in the legs and progresses to the arms, but it occasionally begins in the arms or head.
- In 90% of patients, weakness is usually maximal at 3 to 4 weeks. Deep tendon reflexes are lost. Sphincters are usually spared. Weakness remains the same for a variable period of time, typically for a few weeks, then resolves.
- Facial and oropharyngeal muscles are weak in > 50% of patients with severe disease. Dehydration and undernutrition may result. Respiratory paralysis severe enough to require endotracheal intubation and mechanical ventilation occurs 20%
- A few patients (possibly with a variant form) have significant, life-threatening autonomic dysfunction causing blood pressure fluctuations, inappropriate antidiuretic hormone secretion, cardiac arrhythmias, gastrointestinal stasis, urinary retention, and pupillary changes.
- An unusual variant (Fisher variant, or Miller-Fisher syndrome) may cause only ophthalmoparesis, ataxia, and areflexia.
Diagnosis
- CSF analysis may detect albuminocytologic dissociation (increased protein but normal white blood cell count), but it may not appear for up to 1 week and does not develop in 10% of patients.
- Intensive supportive care
- IV immune globulin (IVIG) or plasma exchange
- Guillain-Barré syndrome is a medical emergency, requiring constant monitoring and support of vital functions, typically in an intensive care unit. Forced vital capacity should be measured frequently so that respiration can be assisted if necessary; if vital capacity is < 15 mL/kg, endotracheal intubation is indicated. Inability to lift the head off the pillow by flexing the neck is another danger sign; it frequently develops simultaneously with phrenic nerve (diaphragm) weakness.
- If oral fluid intake is difficult, IV fluids are given as needed to maintain a urine volume of at least 1 to 1.5 L/day. Extremities should be protected from trauma and from the pressure of bed rest.
- Heat therapy helps relieve pain, making early physical therapy possible. Immobilization, which may cause ankylosis and contractures, should be avoided. Passive full-range joint movement should be started immediately, and active exercises should be initiated when acute symptoms subside. Low molecular weight heparin (LMWH) helps prevent deep venous thrombosis in bedbound patients.
- Given early, IVIG is the treatment of choice. It can be given in one the following ways:
- IVIG 2 g/kg over 1 to 2 days, with acetaminophen 650 mg and diphenhydramine 25 mg given orally 30 minutes before
- IVIG given more slowly, as 400 mg/kg IV once a day for 5 consecutive days
- Plasma exchange helps when done early; it is used if IVIG is ineffective. Plasma exchange shortens the disease course and hospital stay, and reduces mortality risk and incidence of permanent paralysis. However, it may cause hypotension due to large fluid shifts, and IV access may be difficult or cause complications.
- Plasma exchange removes any previously administered IVIG, negating its benefits, and so should never be done during or soon after use of IVIG. Waiting at least 2 to 3 days after stopping IVIG is recommended.
- Corticosteroids do not improve and may worsen the outcome. Eculizumab may be beneficial, but further study is needed before it can be recommended.
CME INDIA Highlight
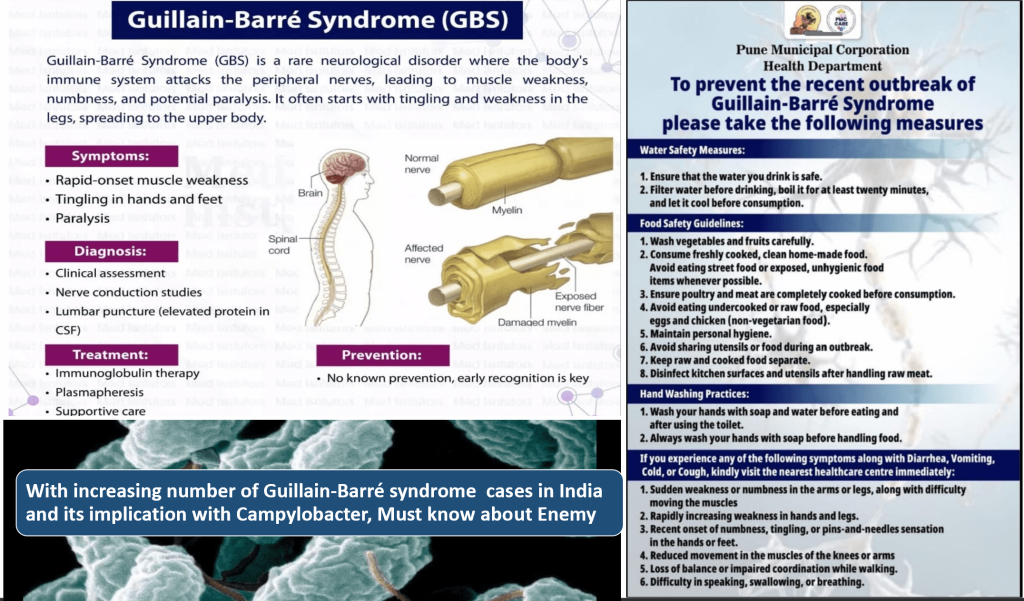
With increasing number of Guillain-Barré syndrome cases in India and its implication with Campylobacter —-Must know Pearls
Key Points About Campylobacter Infection
| 1.Campylobacter is a leading cause of foodborne illness worldwide, with C. jejuni being the most common pathogen in human infections. |
| 2.This bacterium is highly adaptable and can survive in diverse environments. Even small bacterial loads can cause infection. |
| 3.High-risk groups include international travellers, individuals frequently exposed to livestock, and those consuming untreated water or unpasteurized milk. |
| 4.Symptoms typically include diarrhea (sometimes bloody), peaking 1-2 days after onset. The acute enteritis phase is usually self-limiting, resolving within 7 days. |
| 5.Diagnosis is confirmed through stool culture, PCR, or enzyme immunoassay (EIA). |
| 6.Most cases are self-limiting, requiring only supportive care with fluids and electrolytes. If antibiotics are necessary, azithromycin is the preferred treatment. |
| 7.Complications can occur, including an association with Guillain-Barré syndrome. |